
While the total number of contraceptive prescriptions in the UK* has decreased, the pill remains the most commonly prescribed method, new data has shown.
The data, obtained from the NHS Business Services Authority via a Freedom of Information request, shows the total number of contraceptive prescriptions decreased by more than 15% between the financial years 2015/2016 and 2022/2023.
The data reveals that the contraceptive pill — the first iteration of which was invented more than 60 years ago — remains the most commonly prescribed contraceptive method.
There are two types of contraceptive pills. The progestogen-only pill, often called the ‘mini pill’, contains a synthetic version of sex hormone progesterone, which the body produces naturally.
The combined hormonal pill contains synthetic versions of both sex hormones progesterone and oestrogen.
Different pharmaceutical companies manufacture different versions of those pills, using different synthetic hormone types and quantities, hence there are so many different pill names.
The chart below shows the top three most commonly prescribed contraceptives each year.
Various contraceptive pill brands comprise the top three most popular methods for all but three years.
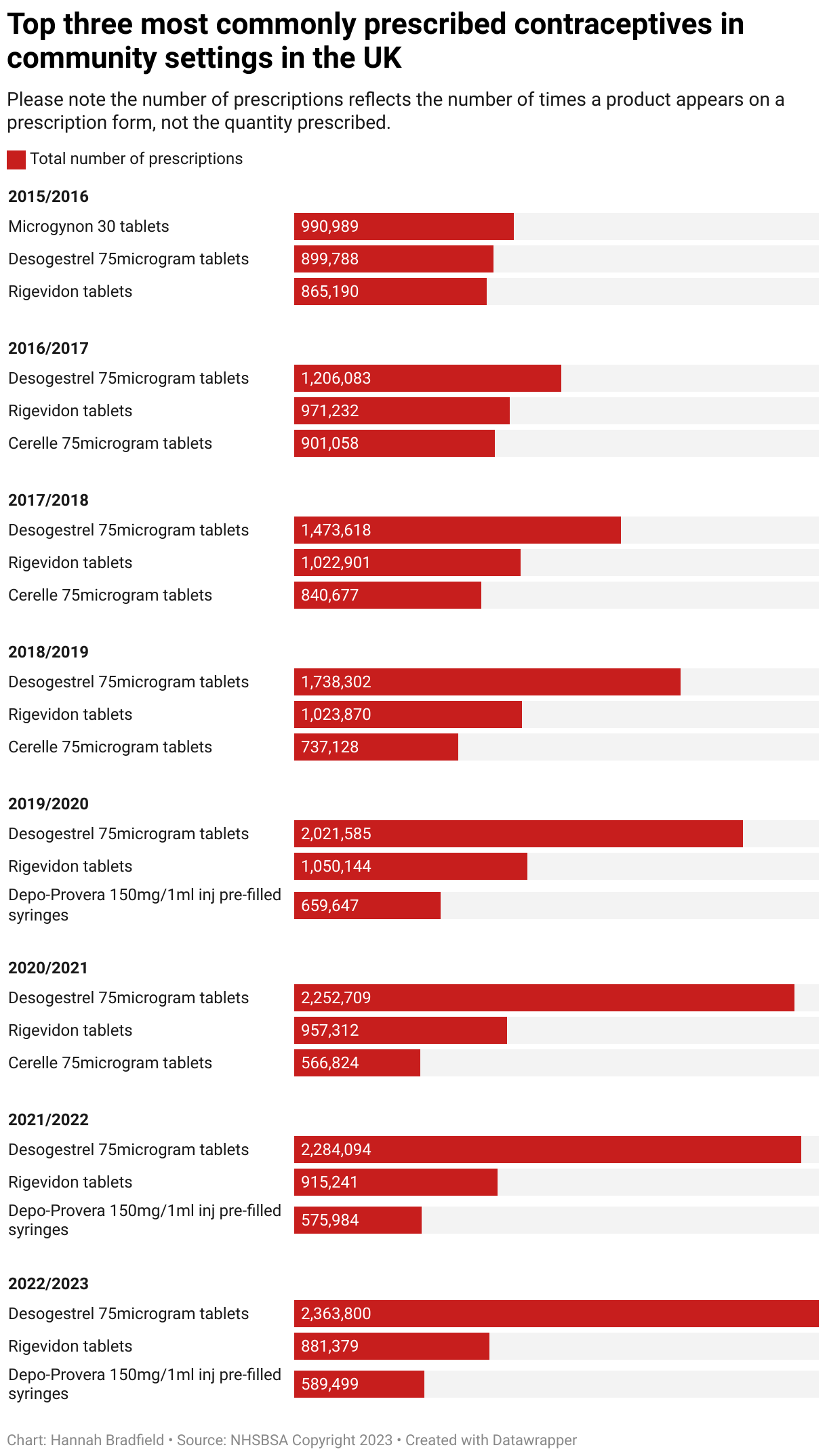
Desogestrel 75 microgram tablets and Cerelle are versions of the progestogen-only pill, while Microgynon 30 and Rigevidon are combined contraceptive pills.
Why is the pill still so popular and what are the issues?
Dr Francis Yarlett is an NHS GP and medical director at The Lowdown, a women’s health review platform providing women with contraception information and advice.
She said: “If you’re looking to go on contraception for the first time, and you’ve got the type of relationship where you can speak to your mum about it, your mum will know about the pill because more often than not, it was what they were on as well.”
The pill is also easy to stop and start, she explained, whereas having something removed from your body is more difficult.

Yarlett added that a lack of funding and training in the GP space can also create barriers to accessing other options.
She explained: “The vast majority of contraception is done by GPs, and in the GP curriculum, there is only a very small amount of time that can be dedicated to contraception.
“So, unless, like myself, you’ve got a real special interest and you go out and train yourself and learn a lot more, you may not be aware of all the different methods.”
Emily Slade, 32, is someone who didn’t know about contraceptive methods that weren’t the pill.
The podcast producer said her GP first prescribed her the combined contraceptive pill aged 17.
Emily continued with it until she got to university, where she was prescribed a different version of the combined pill.
However, after suffering a blood clot, she stopped taking it immediately.
While there were discussions about increased blood clot risk with the combined pill, Emily said it didn’t ever feel particularly serious.
She added: “Whilst I was taking the combined pill, I only ever got told I might get blood clots, I never got told there were other options available to me.
“You don’t listen because you are 17 and just desperately trying to not get pregnant. Skip to 2020, I’ve got a blood clot and taken immediately off the pill. Turns out I was susceptible to them regardless.”
The Lowdown has published a comprehensive guide to blood clots and birth control, highlighting the differences between baseline and increased risk associated with different types of contraception.
Emily said her contraception appointments were quite formulaic.
She explained: “You would go to have your blood pressure taken, it would be perfect, then they would say there is a risk of blood clots.
“When I did get one, suddenly your brain flashes back to every time a doctor mentioned the words ‘blood clot’, and you’re like, ‘how could I be so stupid, they always warned me’.”
“Even after being put on blood thinners, I was told quickly and generically about my other options and to seek out more information if I wanted to consider any but that I could never go back on the combined pill again.”
Cost and funding
Dr Anatole S Menon-Johansson is a clinical lead for sexual health at Guy’s and St Thomas’ and the clinical director at young person’s sexual health and wellbeing charity Brook.
He highlighted another cost issue relating to the reimbursement of GP surgeries fitting LARCs (Long-Acting Reversible Contraceptives).
He said: “You would think that as training goes up, there would be more implementation. But it turns out a lot of GPs are not doing LARC anymore because they’re not reimbursed sufficiently.”
Menon-Johansson says this can push provision onto sexual health clinics, which people are also struggling to access.
According to a recent analysis by the Local Government Association (LGA), which represents councils responsible for public health across England and Wales, sexual health services are at breaking point.
The LGA found that between 2015 and 2024, the public health grant received by councils has reduced in real terms by £880 million (based on 2022/23 prices).
It claims council spending on contraception has suffered as a result.
Yarlett, who has witnessed this first hand, said: “The funding has been cut so much to sexual and reproductive health services in recent years that there isn’t that funding for clinicians to upskill and train themselves, and there aren’t enough clinicians to train other clinicians to do it.
“So we’re stuck in a bit of a cycle.”
Fitting an implant or coil, she says, would require a clinician and assistant, taking more time and resources, whereas to prescribe the pill, you may only need a 10-minute appointment.
However, Yarlett clarifies that ease of access doesn’t mean the pill is not a good option for many people.
The benefits of hormonal contraception like the combined pill, she said, can be huge.
She added: “It treats acne, it treats PMS and PMDD, it treats endometriosis. It treats heavy, painful periods that aren’t endometriosis, and it gives women control over their bleeding.
“It actually reduces the risk of colon, ovarian, and womb cancer. A lot of people don’t know that.”
The importance of choice and education
What is vital, Yarlett and Menon-Johansson both emphasise, is choice.
Contraception services, Menon-Johansson says, need to be supportive, non-judgmental, and have well-trained staff able to deliver all the methods.
He explained: “That is what we try to do at Brook, make sure that all our staff are well-trained in all the methods so we can have that conversation, support women to make those decisions at the right time, and make changes when it’s appropriate.”
Yarlett also highlights a sex education system she claims is not fit for purpose.
While it teaches you the basics early on, she feels it doesn’t go much beyond that.
She said: “You need another refresher post-16 to go into more depth and be like, okay, so now actually a lot of you are on the pill or the implant, let’s talk about it in more depth. Then again, when you’re a bit older.
“You need to have different levels of information at different parts of your reproductive life cycle.”
Emily wishes she had accessed more information earlier on.
After being prescribed blood thinners, she contacted the GP and specifically asked to discuss contraceptive options when booking.
This time, Emily said she had an incredibly helpful doctor who explained a lot and suggested alternative options.
One of The Lowdown’s mottos is that it should be easier to get your contraception than it is to get pregnant.
However, Yarlett said: “It’s not really quite often, is it? There are so many barriers, which is why we are thrilled that you can buy the pill from the pharmacy now — the progesterone-only pill — and they are rolling out pharmacists being able to start women on a combined pill as well, which is excellent.”
However, Yarlett hopes this doesn’t reduce the number of women accessing LARCs because the pill does have a higher failure rate due to factors like forgetting to take it.
A slight year-on year decrease in prescriptions for the pill
As this graph shows, there has been a slight year-on-year decrease in prescriptions for contraceptive pills.
However, it is important to consider that the data reflects how often a product appeared on a prescription, not the amount.
For example, one prescription could be for one month of the pill, while another could be for a much longer supply.
Menon-Johansson added: “It is certainly easier now to safely give out the pill in one-year increments.”
Anecdotally, many women have taken to social media to discuss their experiences with the contraceptive pill.
More than 21,000 results appear when you search #Contraception on TikTok. This includes videos of people highlighting positive experiences of coming off the pill, like alleged weight loss.
Users also discussed the Natural Cycles app which is a technologically-advanced fertility awareness method using temperature and tracking users’ menstrual cycles to determine when it’s safe to have unprotected sex.
After Emily spoke to her doctor, she chose the mini pill. However, she stopped taking it after less than three months as she felt like it affected her mood.
She said: “I love the idea of Natural Cycles, but I am absolutely petrified to try it because I’m still adamant about not getting pregnant.”
Emily added she has become more fearful after seeing more people around her experiencing early abortions.
Yarlett said while Natural Cycles could be effective for one person, it might not work for someone else and their lifestyle.
That is why it’s vital, she added, people know how to look for credible sources online.
The ‘controversial’ Rigevidon pill
One contraceptive pill that has faced criticism over the years is Rigevidon, which consistently appears in the most commonly prescribed contraceptives.
This petition calling for Rigevidon to be banned amassed almost 27,000 supporters.
The death of one 21-year-old woman, Fallan Kurek, in 2015 received considerable media attention, after the contraceptive pill was named as her cause of death. She had been taking Rigevidon at the time.
However, Yarlett stresses the importance of recognising certain biases, adding that Rigevidon is consistently one of the prescribed pills because it is the safest combined pill.
Yarlett explained: “It has the lowest blood clot risk out of all the combined pill brands because of the progesterone that’s in it.
“The reason it gets so much bad press, is because it’s the first one everyone gets put on. So it’s got a negative bias. There is a skew towards the negative side effects because you have got a huge critical mass of women who are taking it. So, a certain percentage of them are going to have side effects and hate it.
“You’ve got a much smaller number of women trying the other pills such as Gedarel, Mercilon, Yasmin, Eloine. So you don’t get as many negative reviews about those because there is not the critical mass.”
The topic can be complex and difficult to understand, which reflects the importance of access to adequate sexual and reproductive healthcare.
So far, nothing has worked for Emily, which she says has prompted her to learn more about her body and menstrual cycle.
In the meantime, however, she added: “I’m very much sticking to condoms.”
*The data represents products prescribed and dispensed in the Community, which includes GP surgeries, pharmacies, and sexual health clinics.
The total number of prescriptions reflects the number of times a product appears on a prescription form, rather than the quantity prescribed.
It covers items prescribed in England that are then dispensed in the community in England, Scotland, Wales, Isle of Man, and the Channel Islands.
Featured image Reproductive Health Supplies Coalition via Unsplash




